Medication reconciliation is a process performed by healthcare professionals where two or more medication lists are compared in order to identify medication errors. Think Research’s MedRec digitizes this previously paper-based medication safety process.
As the primary designer for MedRec, it was crucial for me to have a deep understanding of the safety process, users, and business goals; validate design ideas early and often with clinicians and internal teams; and ensure new features solved real problems.
Product redesign started in 2016 while employed at Think Research.
User InterviewsA/B TestingSecondary ResearchStrategyInformation ArchitectureUser ExperienceInteraction DesignUser Interface DesignMotion Design
The Challenge
When I joined Think Research in 2016, the company was struggling to sell MedRec to other hospitals. The proof-of-concept (PoC) was built too specifically for one pilot hospital and did not scale. In an effort to sell the product to other Canadian hospitals, expand their product offering, and remain competitive, Think Research undertook a full redesign.
The Research
Before jumping into the redesign, I had to understand the domain. I read a lot of ISMP guidelines and other resources to develop a foundational understanding of the medication reconciliation process.
Through site visits to hospitals, interviews with 22 different clinicians, and secondary research, I learned that:
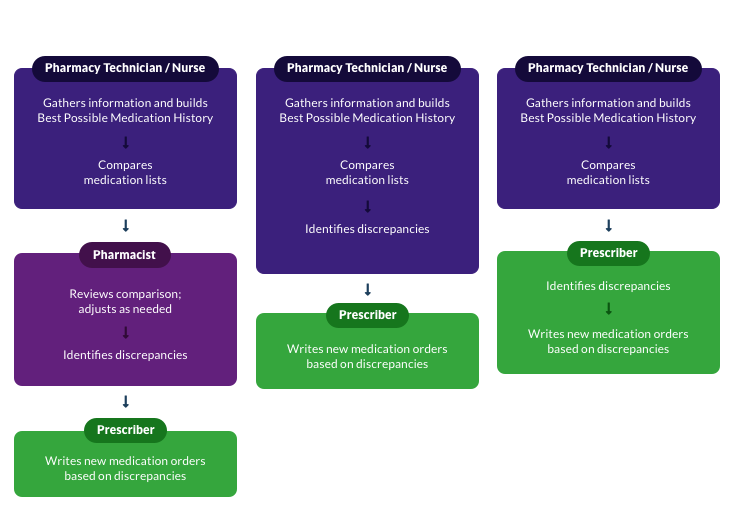
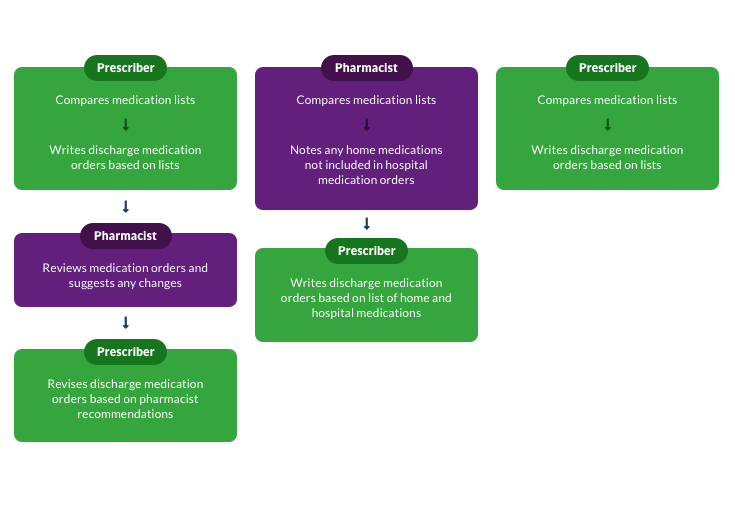
1) Every hospital is different
Medication reconciliation workflows are not standardized across hospitals and departments in Canada. Responsibilities and procedures vary widely between roles. The redesign needed to be flexible enough to accommodate different processes.
2) Efficiency is key
The PoC struggled with adoption. Clinicians complained of long page-load times, too many steps and clicks to complete primary tasks, and too little information being visible at once (as compared to paper). Adoption of the redesign would be difficult if it didn't solve key issues around speed, fatigue, and cognitive load.
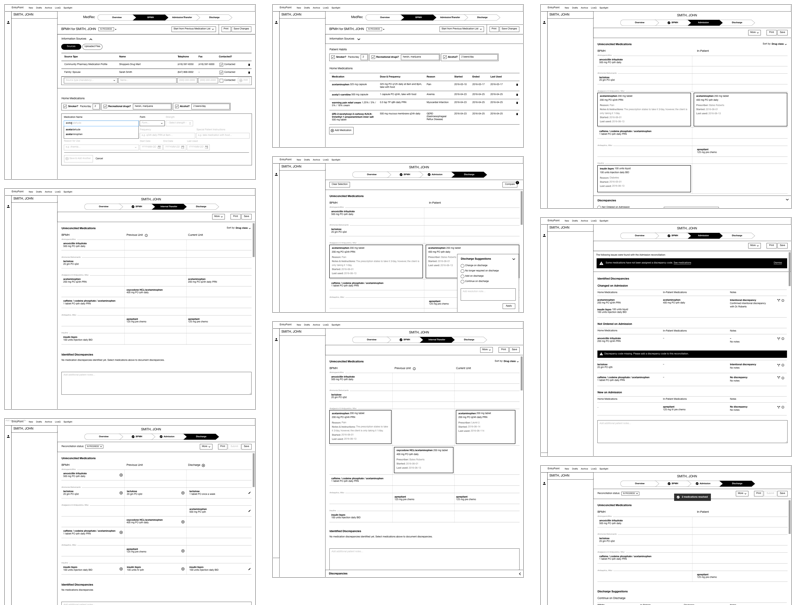
The Redesign
Through cycles of whiteboarding sessions, wireframes, UI designs, testing, feedback and iteration I validated ideas through a clinical lens with in-house and front line pharmacists and physicians.
Together with clinicians and developers, I helped design everything from the product’s layout, flexible workflow logic, unique features, and ISMP features, down to the nitty gritty details like clinical formatting of medication and the design of printed reconciliation reports.
Using my research findings, not only did we redesign the product, but we addressed the primary pain points of the PoC:
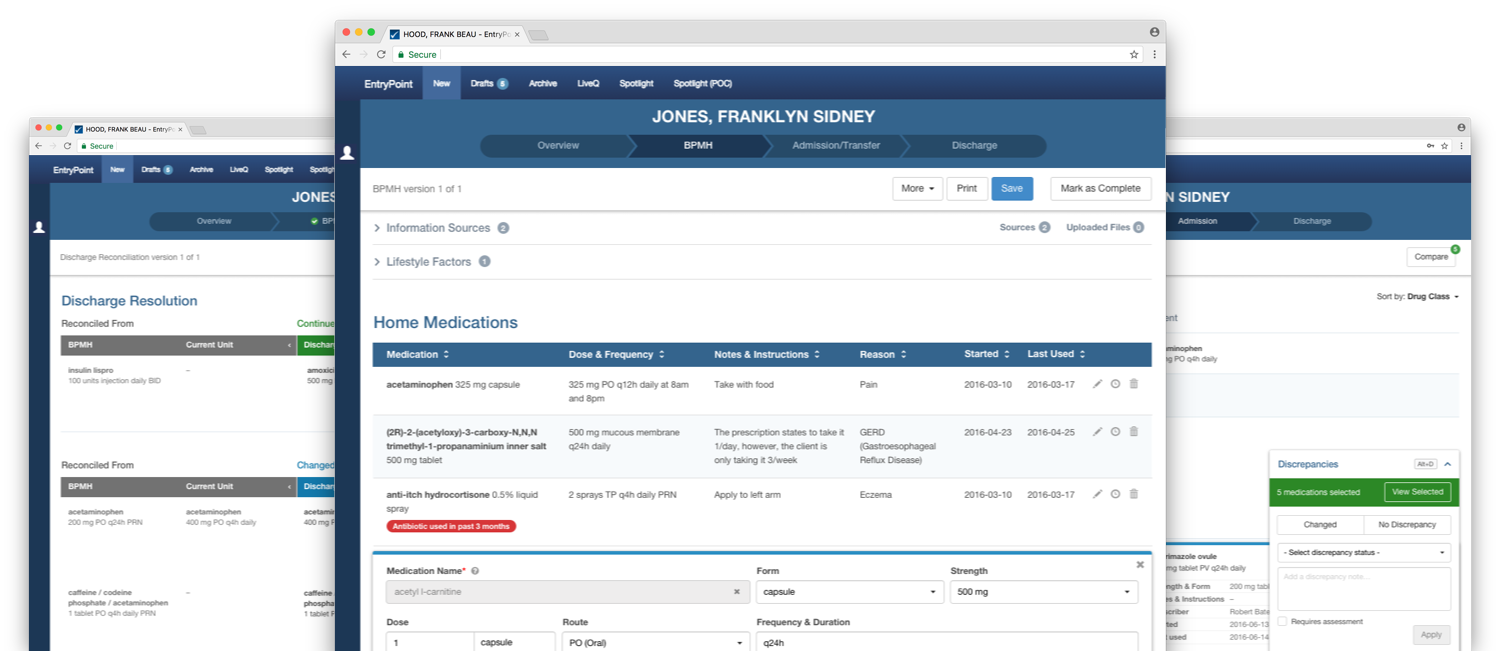
Reduced cognitive load
Less is more
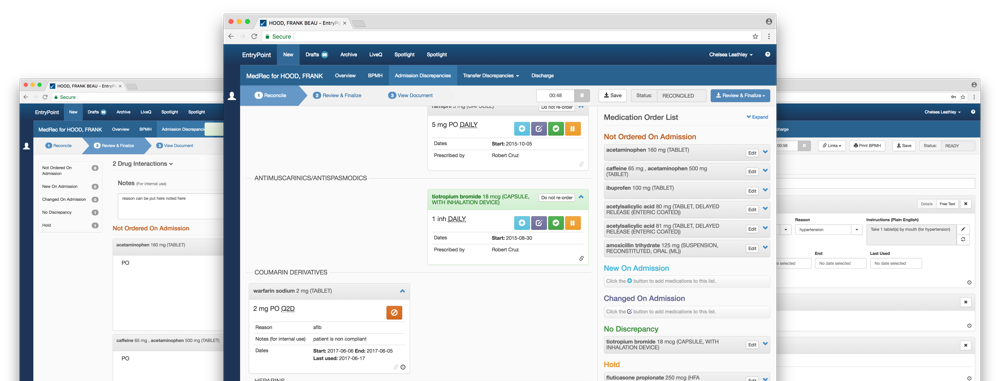
Through user testing and interviews with clinicians, I was able to determine the minimum amount of information a clinician needed to see in order to make a decision about a medication. This increased the number of medications visible at once by 40%, while still allowing clinicians to view more information when needed.
Comparing medications
Comparing medications across the top and bottom of a list in the PoC required clinicians to remember medication details while scrolling. The compare function was designed to allow users to see selected medications next to each other, while hiding any unselected medications. This helped clinicians by reducing the cognitive load required to remember details between medications at the top and bottom of a patient’s medication list.
Faster work with less effort
Keyboard-centric
From the site visits, I found that clinicians were using their keyboard for both input and navigation. Switching between a mouse and keyboard only slowed down their process. To remedy this, tab index order and keyboard shortcuts were introduced in the redesign to address their issues around speed and fatigue.
Single page workflow
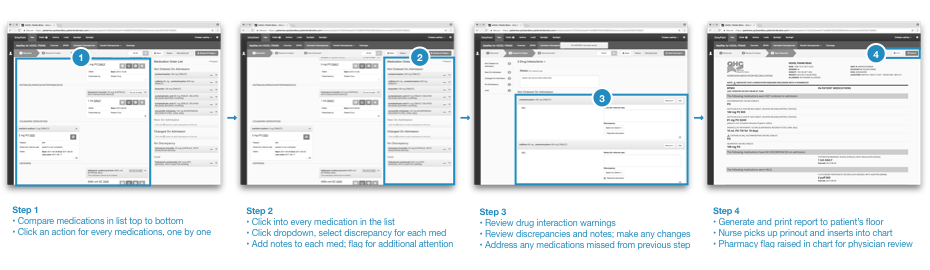
Through collaboration with pharmacists, the PoC’s three-screen process to complete a reconciliation was reduced down to one. This meant that as medication discrepancies were identified, medications would be removed from the list at the top of the page and moved to the table at the bottom of the page. Once all medications had been reconciled, the list would disappear and only the table would remain, making it obvious that all medications had been assessed.
Getting the product to do the heavy lifting
Highlighting similar medications
To improve the speed and workload associated with comparing medications one by one, a developer-pharmacist and I designed a feature that would automatically select all related medications based on a single selection by the user. This meant that the product would do some of the manual and mental work for the user by identifying similar or related medications using the medication name, form and route and mapping it to the enhanced therapeutic class pulled from First Databank.
Smart Actions
To reduce the likelihood of clinician error, I introduced contextual actions. Depending on the combination of medications selected from each list, certain actions become available to the user. In collaboration with a pharmacist, I mapped out all the potential combinations and resulting actions in order to limit the actions presented in the interface and decrease the likelihood of error.
The Result
In two years, the redesign and careful consideration for users’ needs saw MedRec grow from being able to support only one client, to being the choice solution for 2 hospitals in Southern Ontario and the only solution for all acute and long-term care centres in Newfoundland over a five-year rollout plan.
As the lead designer and now a subject matter expert on medication reconciliations, I continue to act as the go-to resource for researching, designing and understanding new and existing features in MedRec.